Lumbar Degenerative Spondylolisthesis
Full-endoscopic Trans-Kambin Lumbar Interbody Fusion (KLIF) for spondylolisthesis
1: Historical perspective
There are variety types of the lumber interbody fusion (LIF). The name of the procedure is made due to the cage insertion anatomical location: ALIF from anterior, PLIF from posterior; XLIF from extreme lateral and so on. Kambin triangle was not the location for the cage insertion, historically. On the other hand, after development of the surgical skill, one can insert a cage through the Kambin triangle.
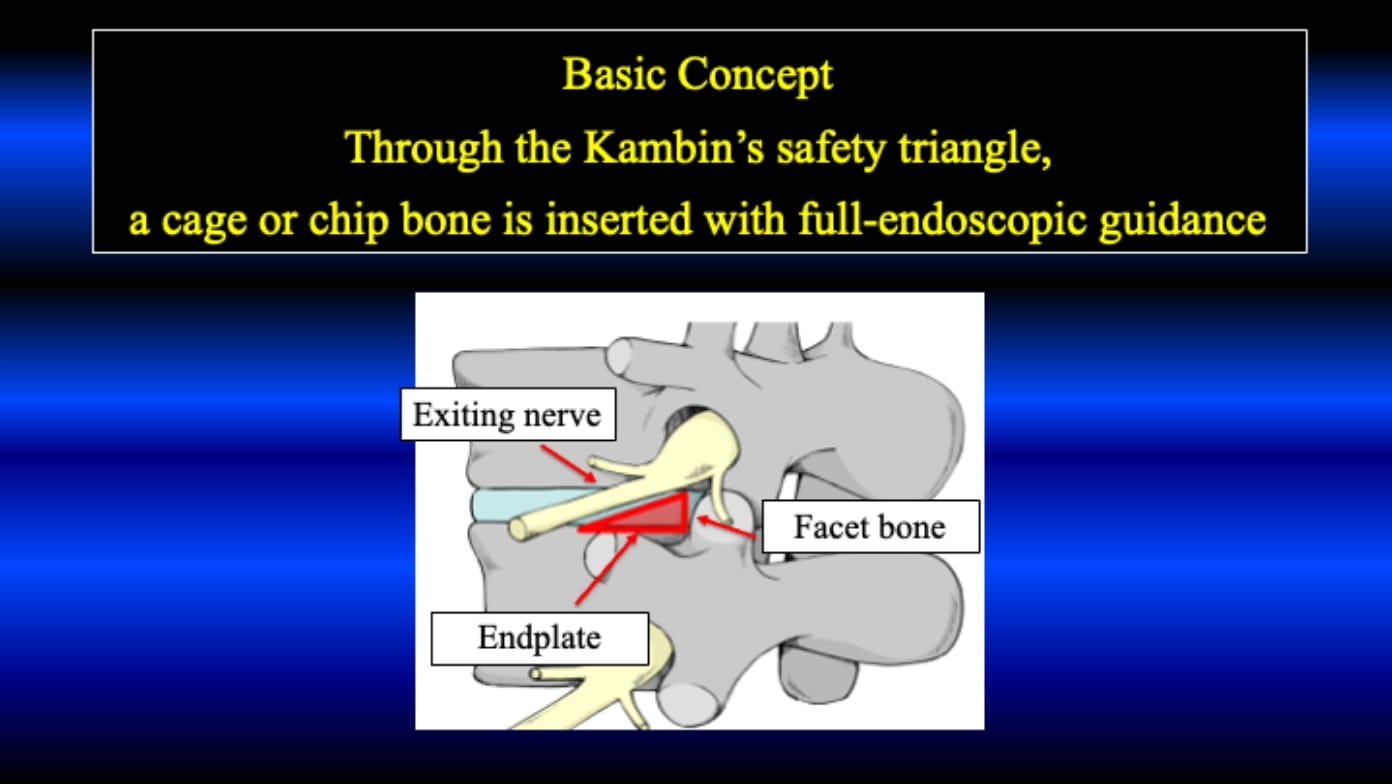
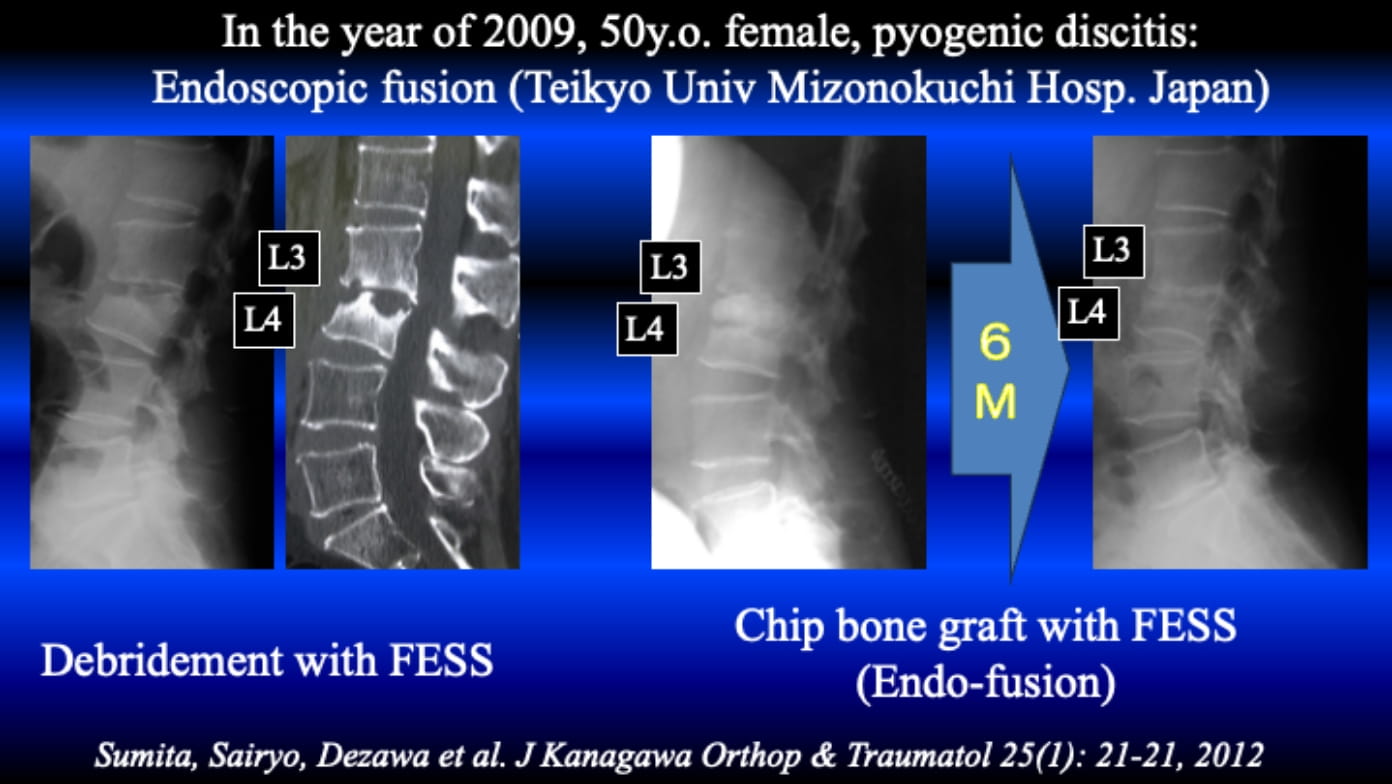
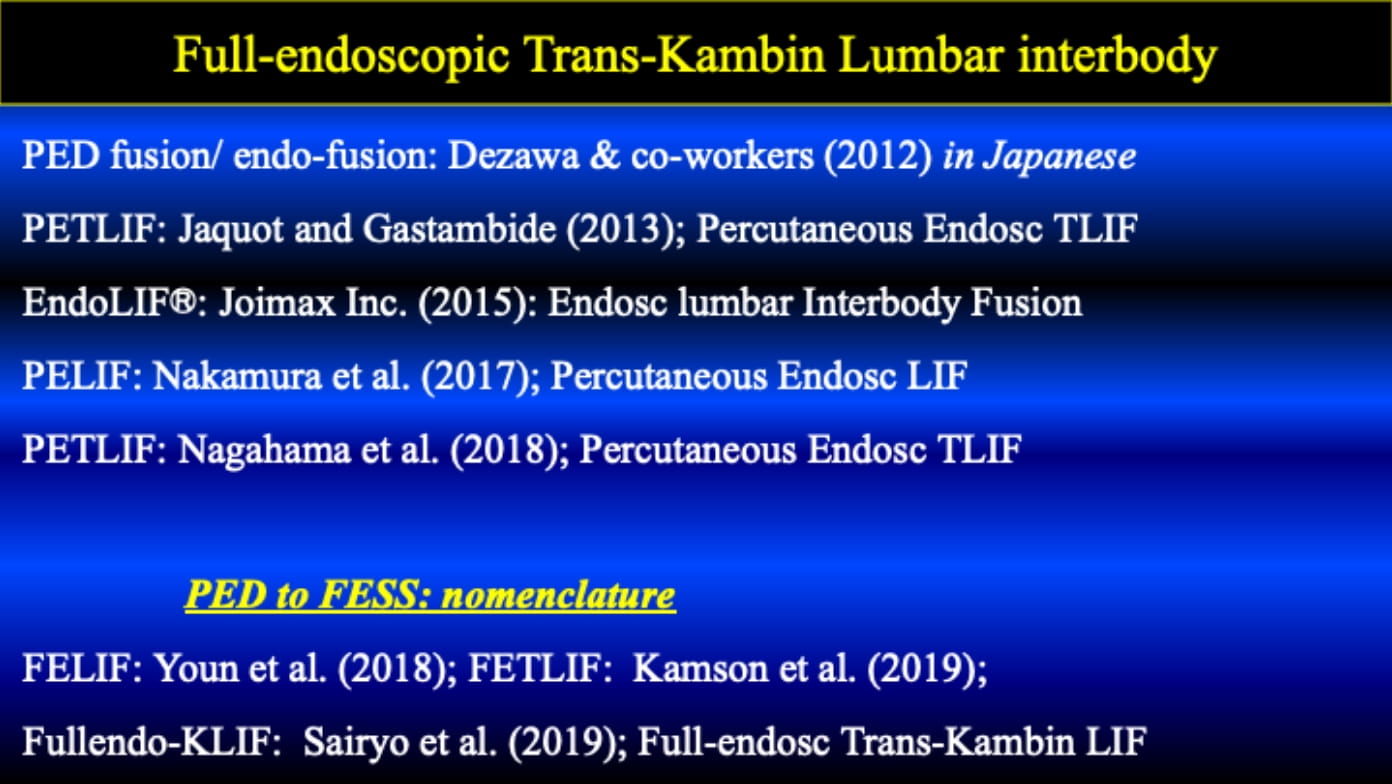
The following case would be the first case in Japan. Full-endoscopic debridement could subside the infection and several weeks later, chip bones were inserted through the Kambin triangle under full-endoscopic guidance in 2009. They called PED-fusion or endo-fusion at the time. They did not use a cage and percutaneous pedicle screws.
After 2013, percutaneous pedicle screws and cages started to use for the dull-endoscopic fusion. Since then, in the literature, so many reports have been published on the similar technique. The procedure is called as PETLIF, EndoLif, PELIF, FELIF, FETLIF and so one. All procedure is similar as the insertion of the cage through the Kambin triangle; thus, I proposed to use trans-Kambin fusion (KLIF) in 2019.
2: Surgical technique
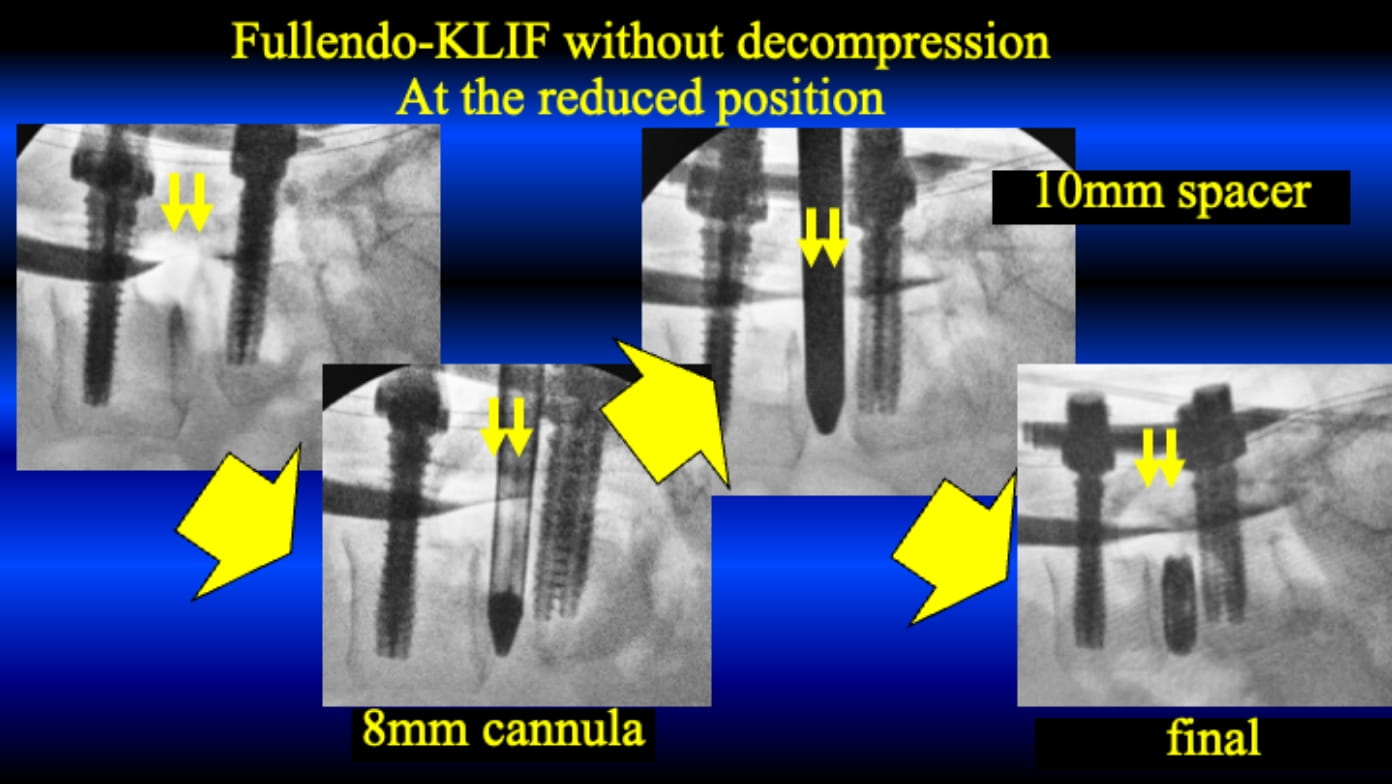
First, we insert 4 percutaneous pedicle screws (PPS) with small skin incisions. Then, using special made open square cannula, a cage is inserted through the Kambin triangle under guidance of the full-endoscope. Usually, it is conducted under general anesthesia.

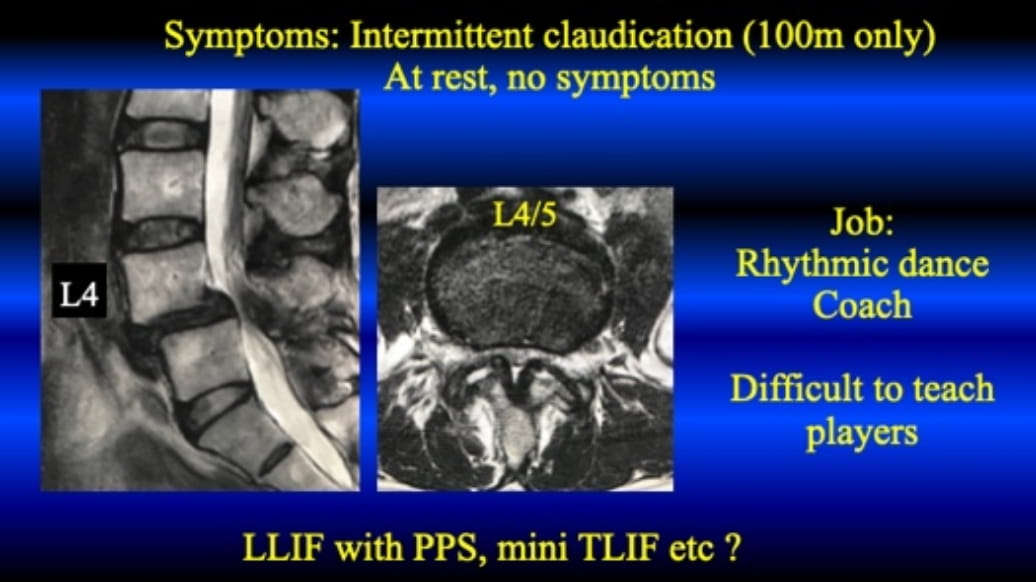
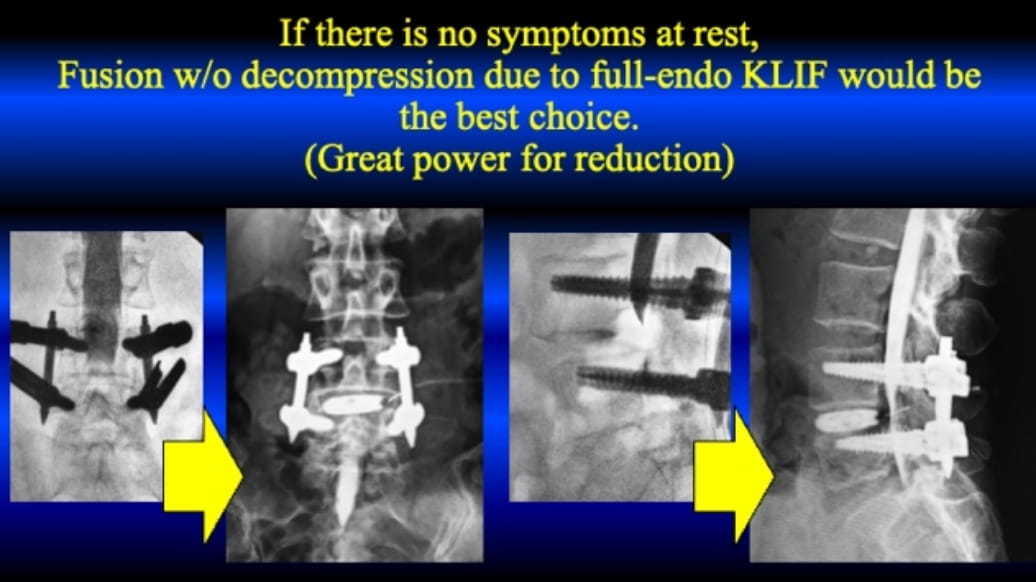
The following case is 57 y.o. female, high school teacher. The slippage in the neutral position is grade I; however, in flexed position it is grade II, almost 30%. Her symptom is just intermittent claudication, and there is no symptom at rest. Thus, FE-KLIF without direct decompression is conducted.
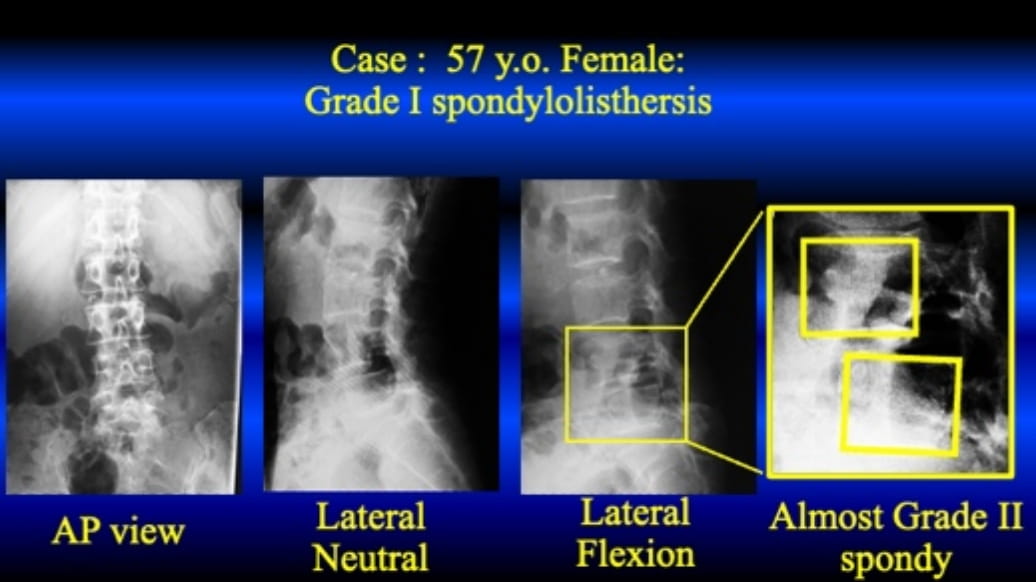
During the procedure, the slippage is reduced step by step. Finally, the slippage is reduced almost 0% being anatomically normal position. Afte surgery, her chief complaint is completely solved; then, she could return to the original activity.
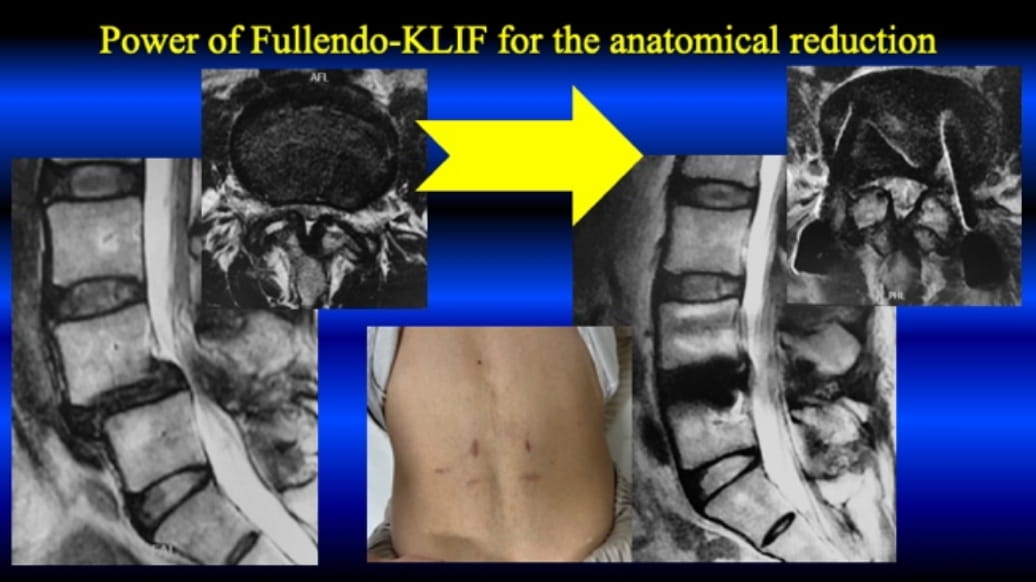
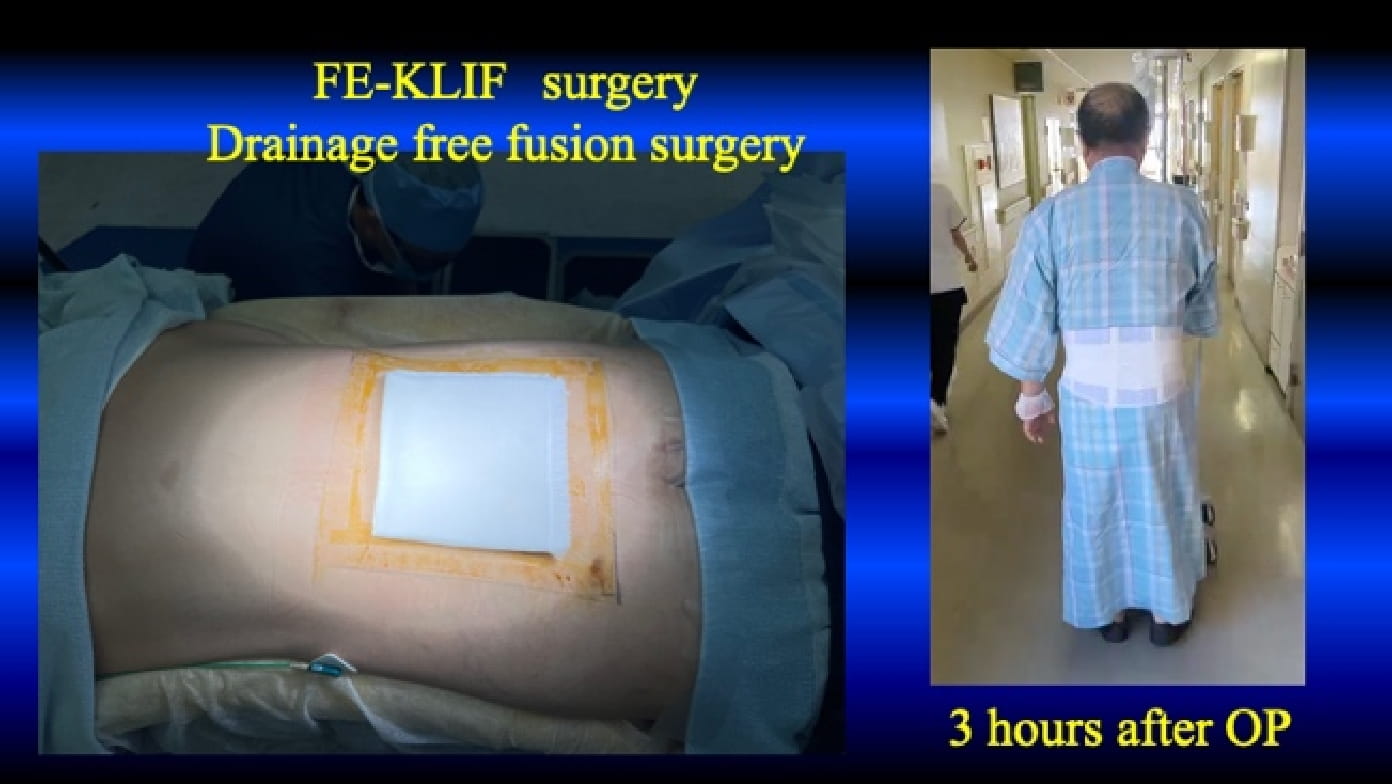
Since FE-KLIF does not require facetectomy and laminectomy, there is no need for worrying about post-surgical hematoma. We do not use drainage after the surgery.
3: Full-endoscopic KLIF under local anesthesia
In some countries in the world, trans-Kambin endo-fusion with PPS has been conducted under local anesthesia. However, in Japan, there is no clinical report on the KLIF under local anesthesia. Recently, we conducted such surgery.
A case is female patient aged over 90. Because of severe leg pain and foot drop, she underwent wide-laminectomy under general anesthesia 5 years ago. The symptom was not improved after the surgery. Since then, the symptoms got worse year by year. Finally, she decided the additional surgery and visited several hospitals for the surgery. However, her age was over 90 years old, and general condition was poor; then, no one agreed the surgery under general anesthesia. She was referred to us. We planned FE-KLIF under local anesthesia.
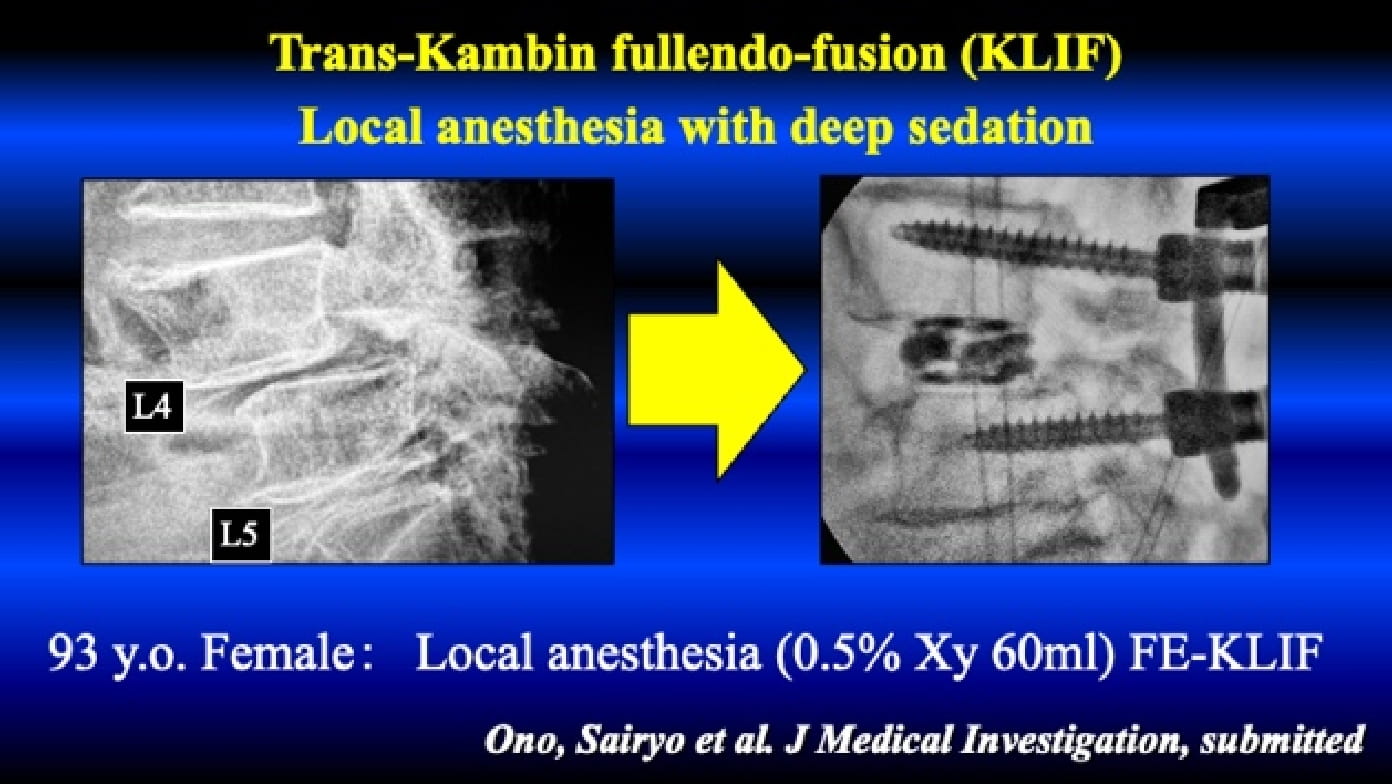
First, we inserted two PPSs from the right side using 20ml of 0.5% lidocaine. Next, trans-Kambin cage insertion was conducted from the left side using 20ml of 0.5% lidocaine. Finally, using the additional 20ml of 0.5% lidocaine, PPSs from the left side were inserted. For this elderly case with poor general anesthesia, FE-LIF was possible under local anesthesia with deep sedation by anesthesiologist.
Current Indication of the FESS under local anesthesia
- Lumbar Herniated Nucleus Pulposus
- Lumbar Spinal Canal Stenosis
- Lumbar Degenerative Spondylolisthesis
- Lumbar Spondylolysis and Isthmic Spondylolisthesis
- Lumbar Tumorous Conditions (Discal Cyst and Juxta Facet Cyst)
- Discogenic Low Back Pain
- Type 1 Modic Change Low Back Pain
- Baastrup Disease (Synovitis and Kissing Spine)
- Thoracic Herniated Nucleus Pulposus
- Thoracic Spinal Canal Stenosis
- Foraminal stenosis
- Central stenosis
FESS and MIS in Sports Medicine
- Lumbar Herniated Nucleus Pulposus
- Lumbar Foraminal Stenosis
- Lumbar Discogenic Pain
- Lumbar Type 1 Modic Change Low Back Pain
- Baastrup disease
- Pars Fracture (Spondylolysis)
Location
Department of Orthopedics, Tokushima University, Tokushima, Japan 3-18-15 Kuramoto-cho, Tokushima-shi, Tokushima 770-8503, JAPAN
Access
Haneda airport to Tokushima airport (1 hour),
Tokushima airport to Tokushima Station (30 min, limousine bus),
Tokushima Station to Tokushima University Hospital (20 min, taxi)