Lumbar Spinal Canal Stenosis
Transforaminal Full-endoscopic Decompression Under Local Anesthesia for Lumbar Spinal Canal Stenosis (LSS):
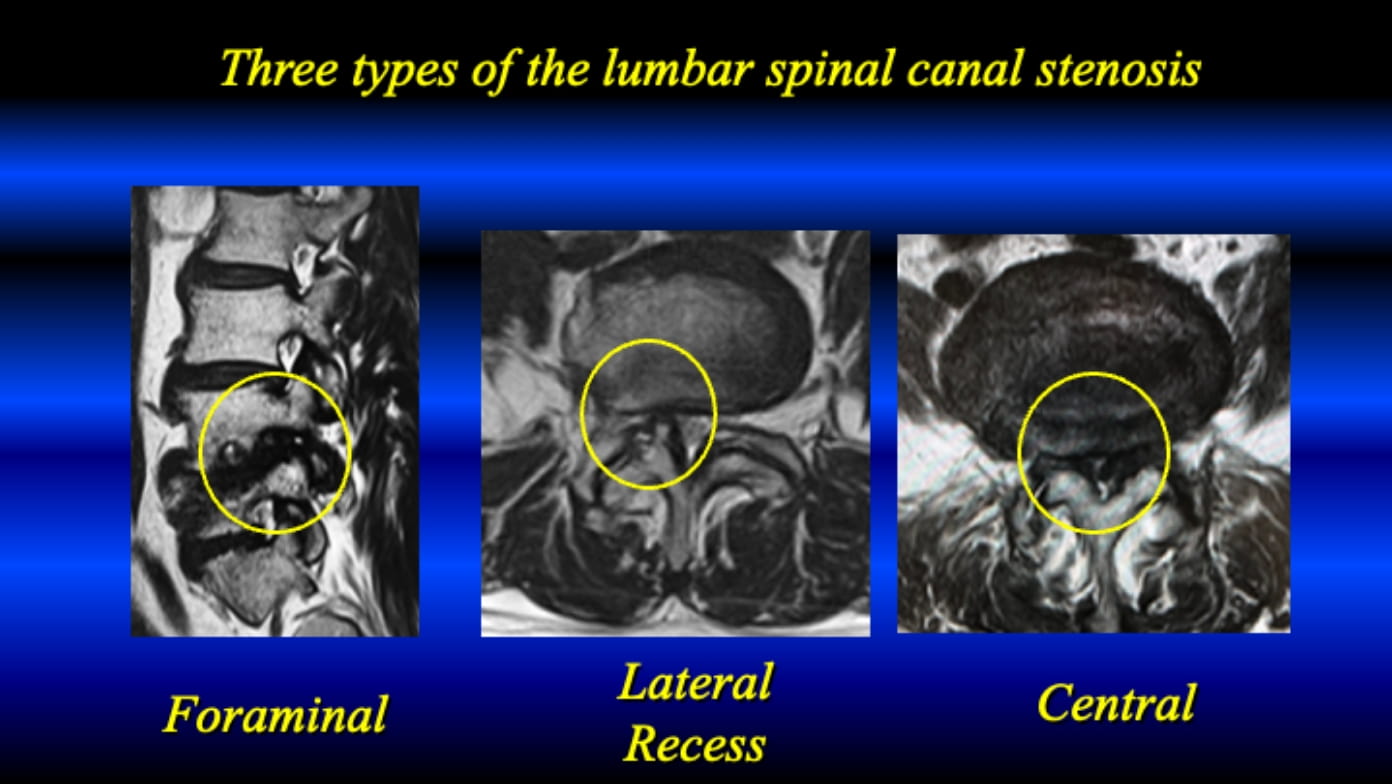
There are three types in the lumbar spinal canal stenosis. The TF-FESS started to decompress the LFF from the pathologies of foraminal stenosis around 2000. The technique of lateral recess decompression with TF-FESS was developed in 2017; then, for central stenosis in 2019.
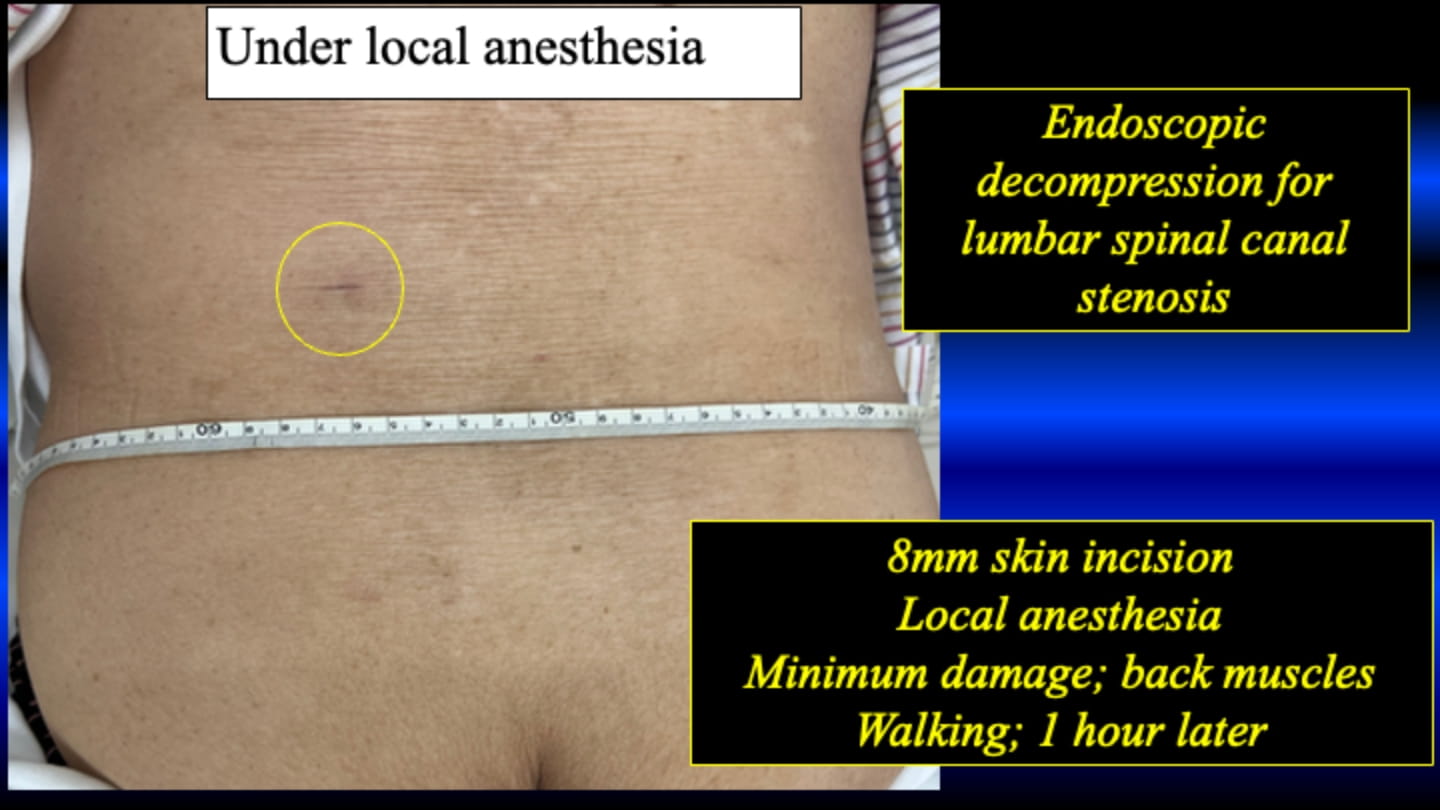
Skin incision is about 8 mm at about 7-10 cm away from the midline of the back.
Please see the below. The TF-FESS surgery under local anesthesia initiated by discectomy of the herniated nucleus pulposus. Now, the procedure can be applied for all three types of the lumbar spinal canal stenosis under local anesthesia.
(1) Lumbar foraminal stenosis
This case is 28 y.o. female professional golfer. She complained severe left leg pain due to HNP at L5/s. The HNP was removed via transforaminal access with FESS following foraminotomy. After the surgery, her leg pain completely disappeared; then, she could return to the original activity 2 months after the TF-FESS.
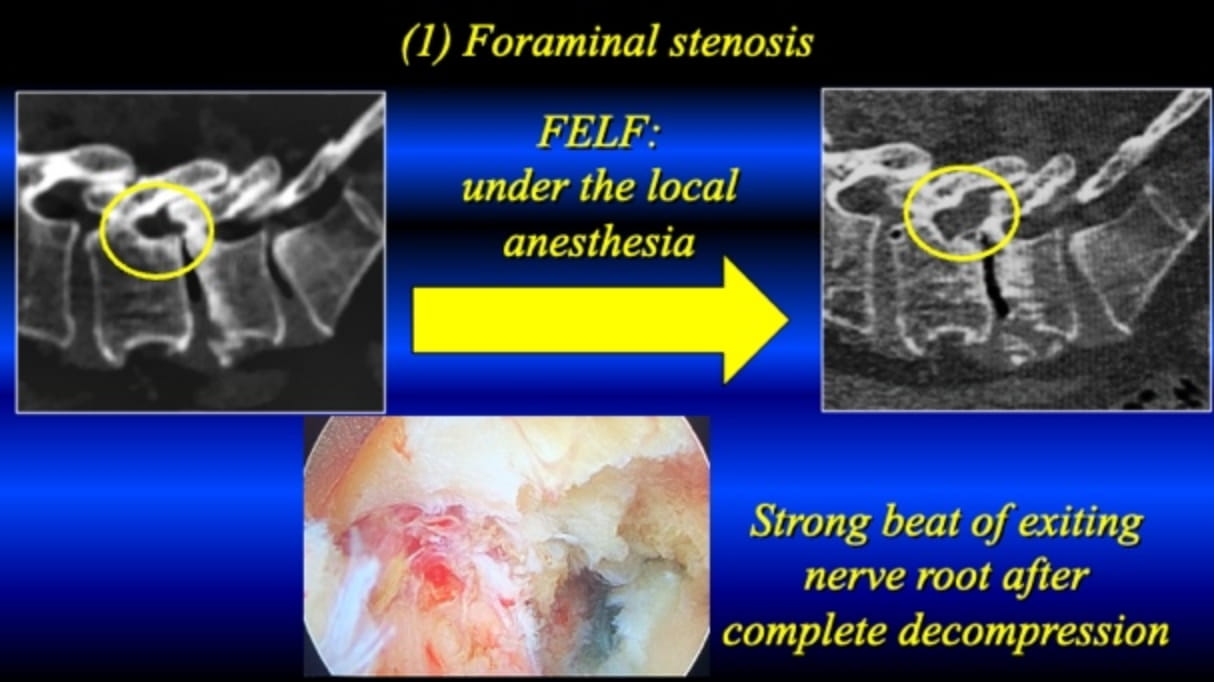
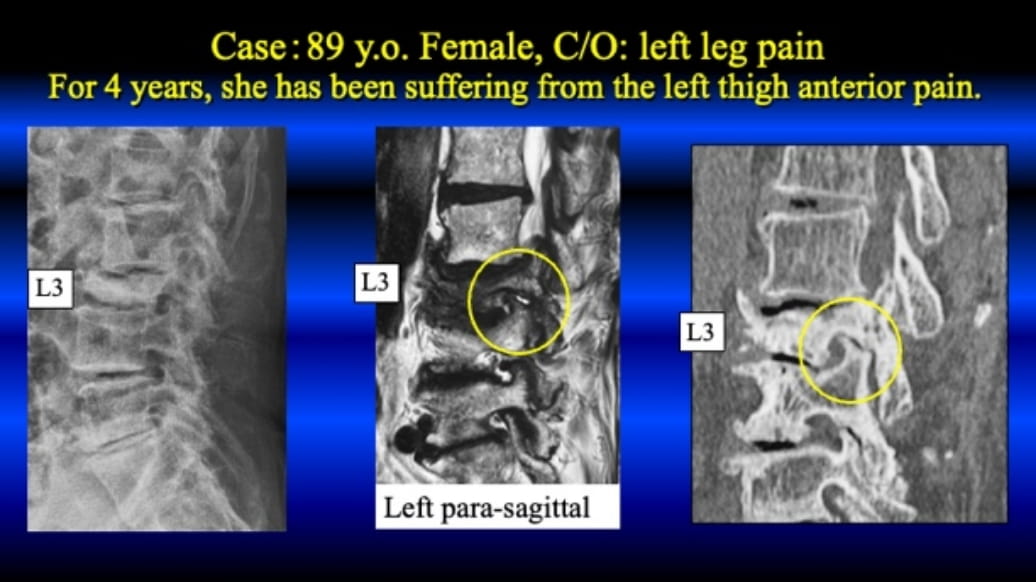
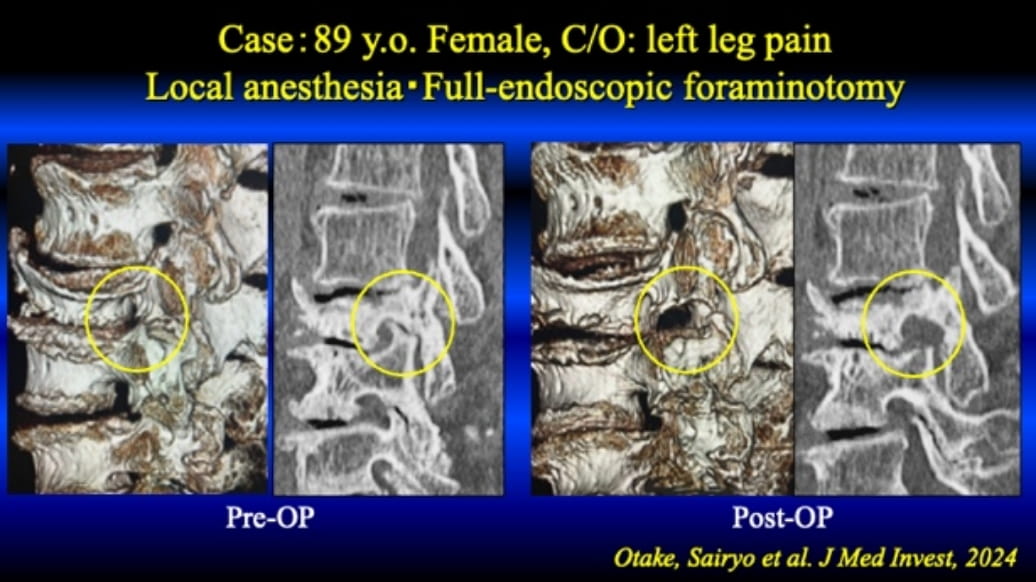
This representable case is a 89 years old female. Four years ago, she had vertebral body fracture, and it was healed with conservative treatment. Although vertebral body was collapsed, severe low back pain was disappeared. Instead, let high pain appeared. Since her cardiac function was very poor, and her age was very elderly, her local surgeons did not recommend surgical intervention with general anesthesia. Then, she was referred to us. Under local anesthesia, her narrow foramen was successfully enlarged by TF-FESS (foraminotomy), and her leg pain disappeared. Please see the figures below, and the circle indicates the change of the foramen before and after surgery.
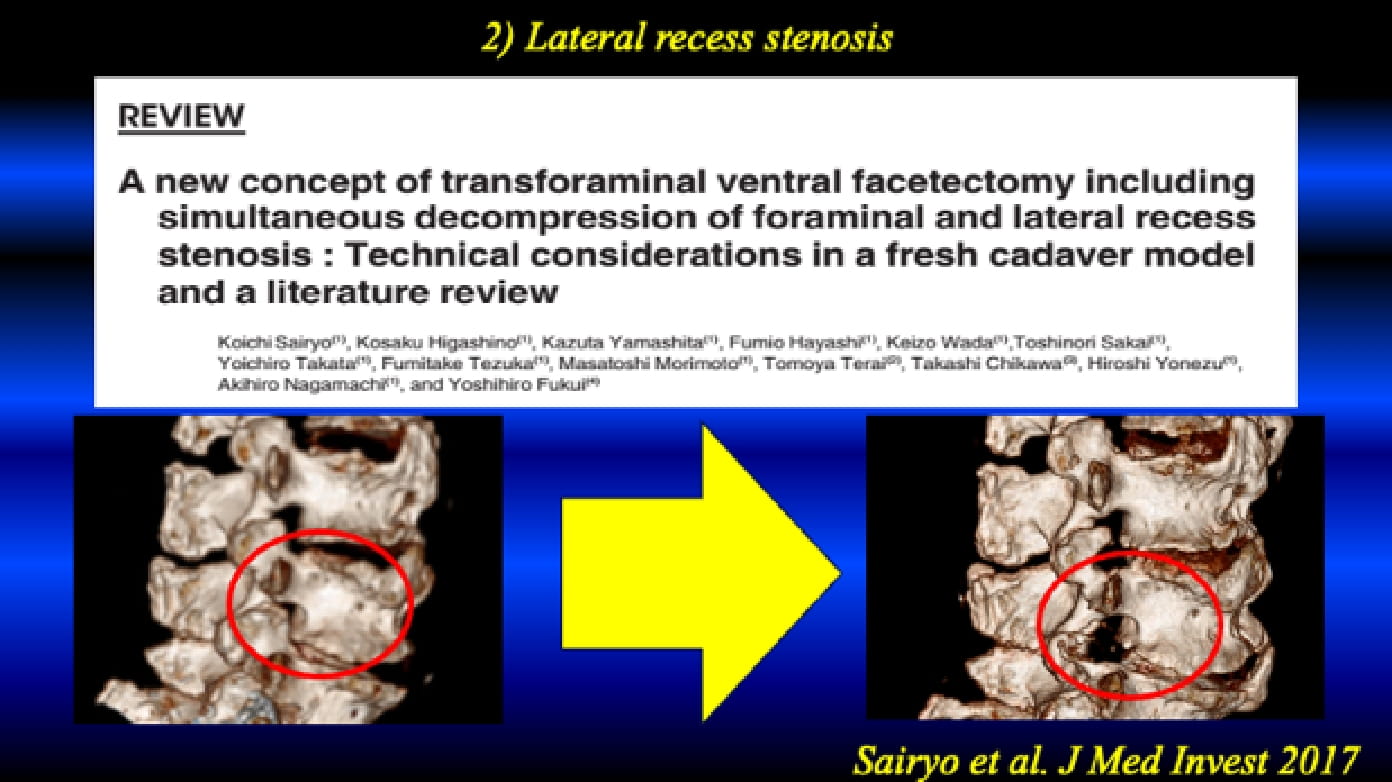
(2) Lumbar lateral recess stenosis
This type of the stenosis is usually decompressed via inter-laminar approach under general anesthesia with or without endoscope. Of course, FESS surgery has been applied for this decompression in these days. In Japan, such a super-aging society, there are many elderly patients with poor general condition. Thus, we should develop the novel surgical technique to decompress this pathology under local anesthesia using TF-FESS. Finally, we could establish the technique to decompress the lateral recess stenosis under local anesthesia in 2017. We named the surgical procedure as Full-endoscopic Ventral Facetectomy (FEVF).
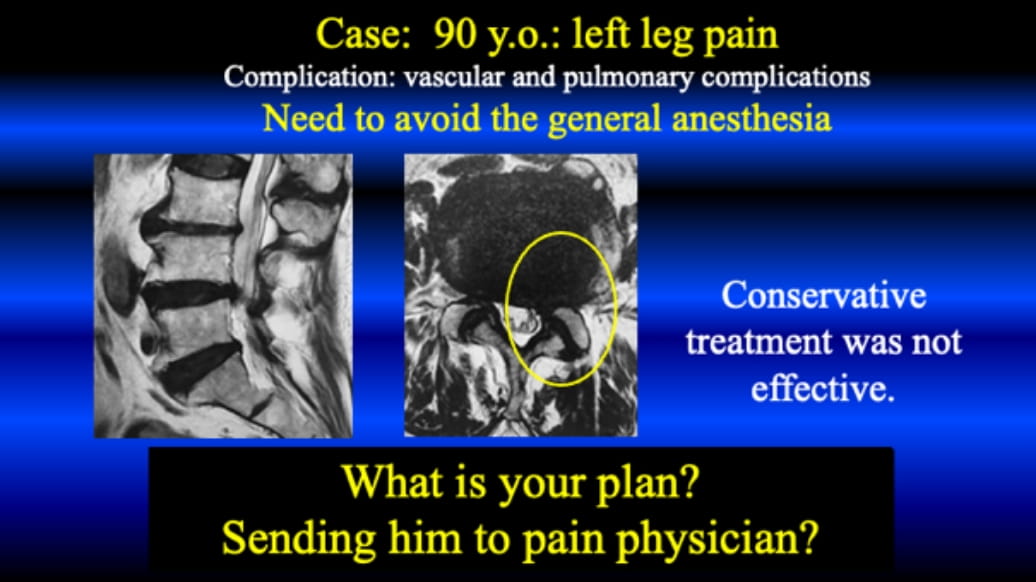
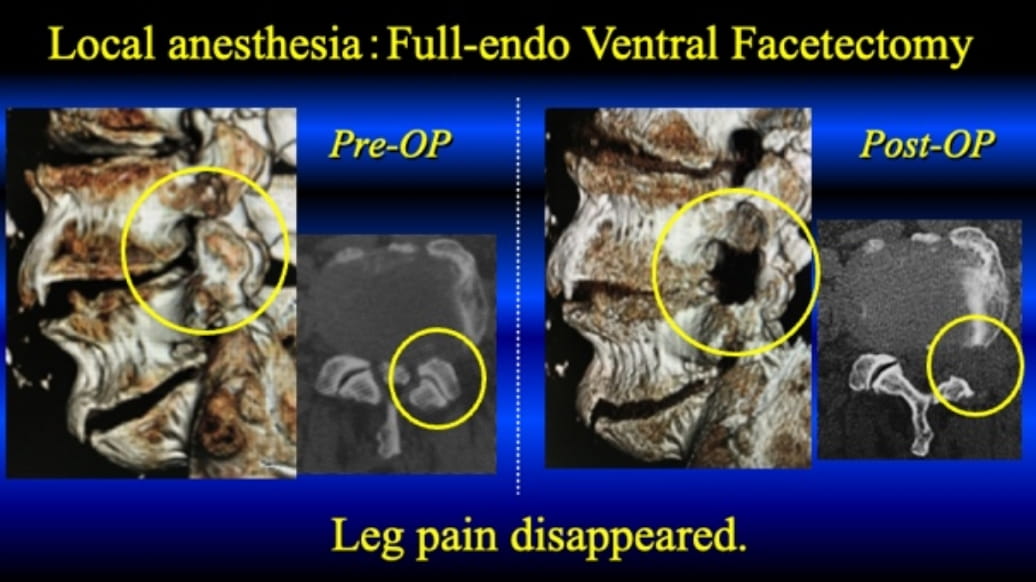
This representable case is 90 years old male. He visited many local doctors with complaining of the left leg pain. Since he is very old (90 y.o.) and he has general complications; thus, no one recommended surgery. He could not tolerate the pain, and he visited us for the purpose of the surgery under local anesthesia. His left leg pain was induced by the lateral recess stenosis, and FEVF was conducted successfully. His symptoms was completely disappeared after the surgery.
This is the final endoscopic view during the surgery. The decompressed L5 traversing nerve root is clearly observed.
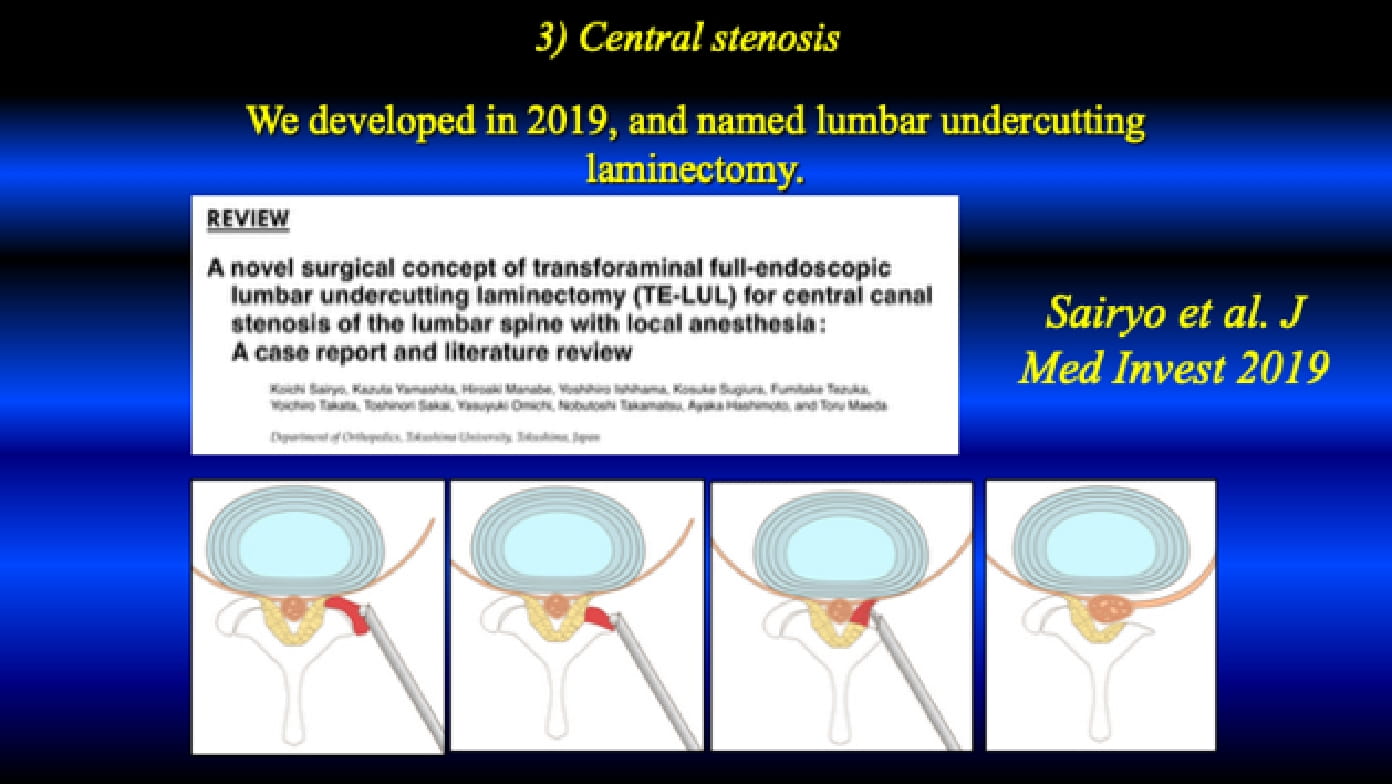
(3) Lumbar central canal stenosis
This type of the stenosis is also decompressed via inter-laminar approach under general anesthesia with or without endoscope as a gold standard surgical intervention.
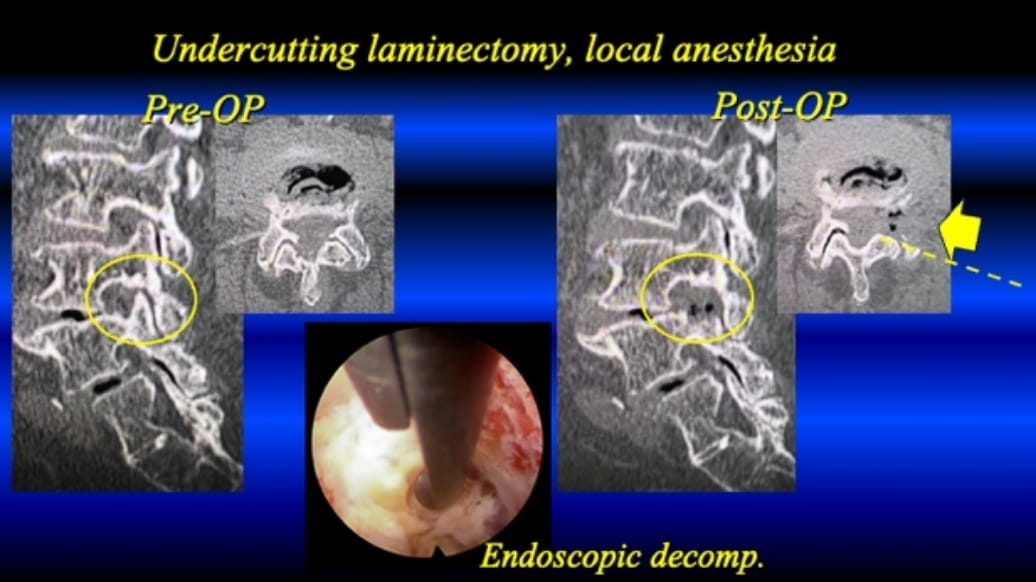
On the other hand, via the transforaminal approach, we developed the technique to decompress the central canal stenosis under local anesthesia. We named the surgical procedure as trans-foraminal endoscopic lumbar undercutting laminectomy (TE-LUL) in 2019. For the bilateral decompression, two staged surgery from right and left side would be recommended due to limitation of the max. dosage of the lidocaine (1%).
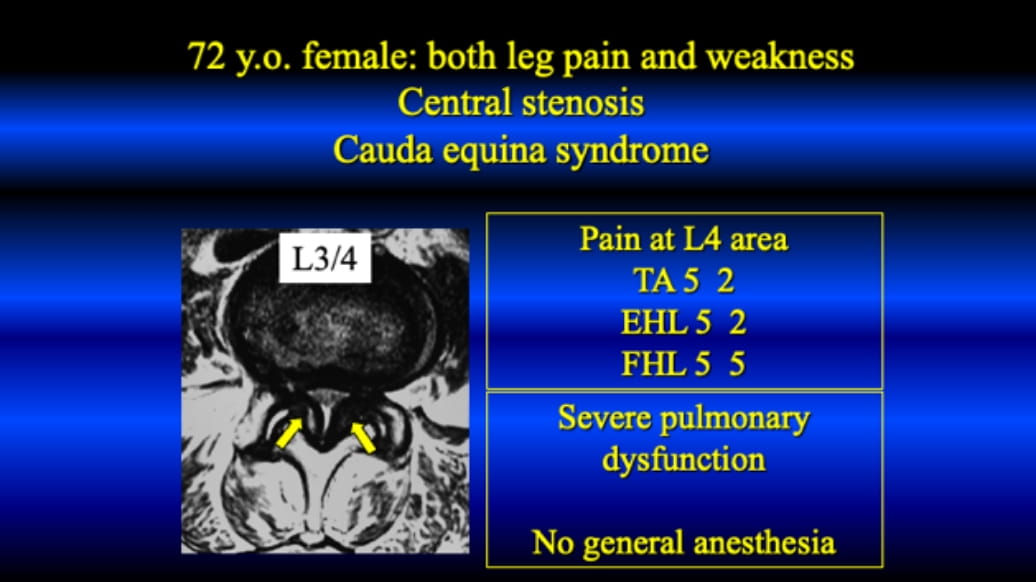
Representable case #1 is demonstrated as below. This is the first case of TE-LUL under local anesthesia in our institution.
This case is 72 years old female, and visited us with both leg pain and muscle weakness at the left side. Interlaminar decompression as ‘laminectomy’ was planned under general anesthesia; however, her pulmonary function was very poor. The laminectomy was cancelled; then, TE-LUL under local anesthesia was conducted instead. After bilateral decompression, her both leg pain was disappeared and the muscle weakness was improved completely within 3 months.

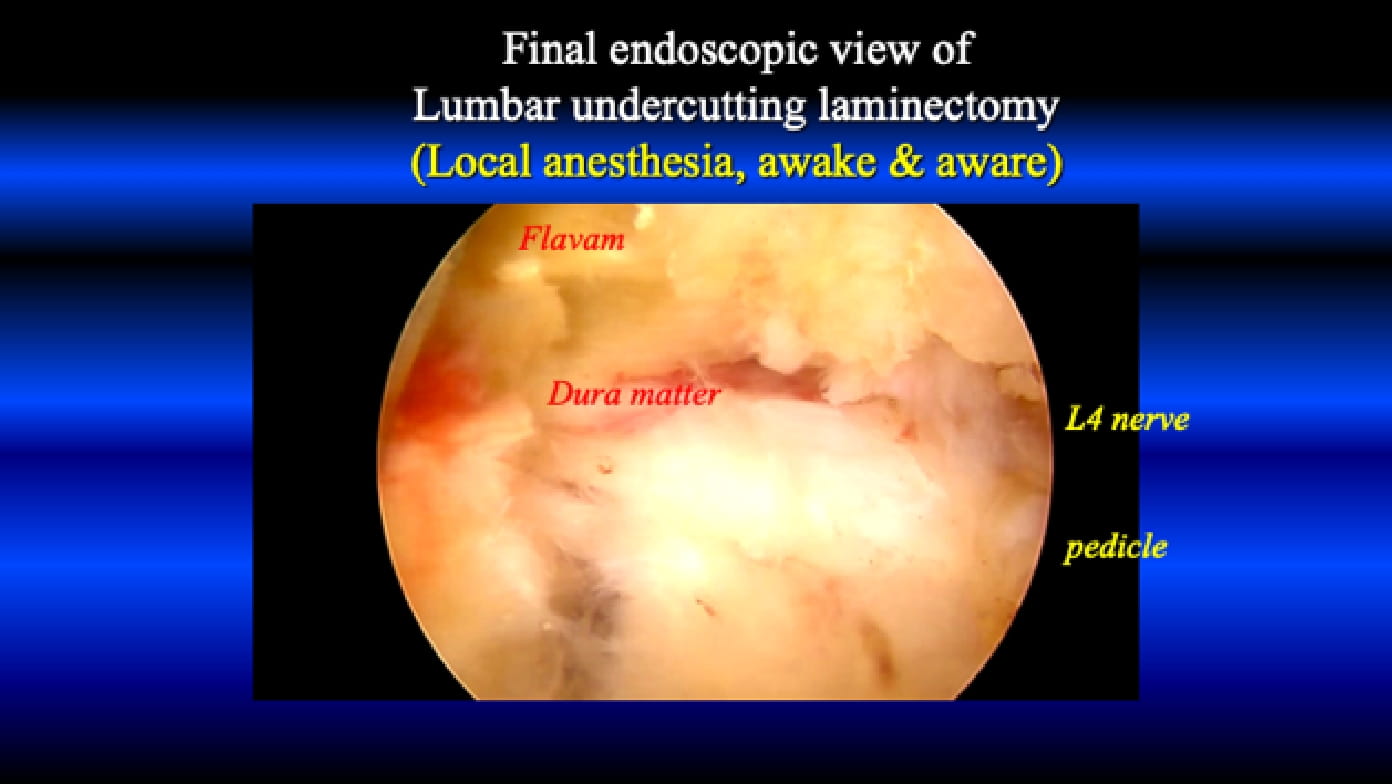
This endoscopic appearance is the final view of the TE-LUL from the left side. The decompressed dural sac is obvious.
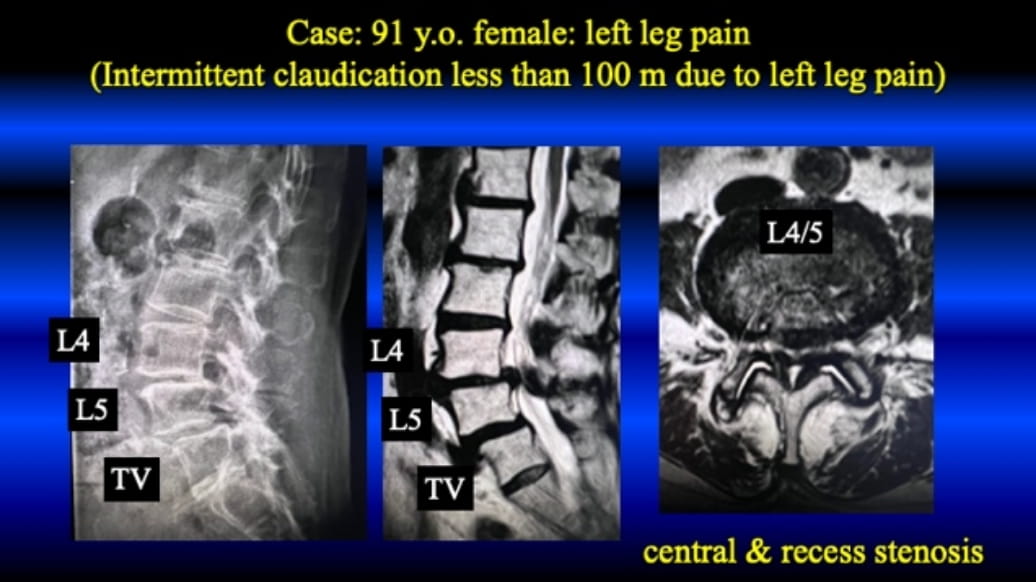
The final case is 91 years old female, and visited us with left leg pain and intermittent claudication within 100 m. Her age was over 90 years old and she was afraid of having the general anesthesia. TE-LUL under local anesthesia was conducted. After left side TE-LUL, her left leg pain was totally disappeared.
Current Indication of the FESS under local anesthesia
- Lumbar Herniated Nucleus Pulposus
- Lumbar Spinal Canal Stenosis
- Lumbar Degenerative Spondylolisthesis
- Lumbar Spondylolysis and Isthmic Spondylolisthesis
- Lumbar Tumorous Conditions (Discal Cyst and Juxta Facet Cyst)
- Discogenic Low Back Pain
- Type 1 Modic Change Low Back Pain
- Baastrup Disease (Synovitis and Kissing Spine)
- Thoracic Herniated Nucleus Pulposus
- Thoracic Spinal Canal Stenosis
- Foraminal stenosis
- Central stenosis
FESS and MIS in Sports Medicine
- Lumbar Herniated Nucleus Pulposus
- Lumbar Foraminal Stenosis
- Lumbar Discogenic Pain
- Lumbar Type 1 Modic Change Low Back Pain
- Baastrup disease
- Pars Fracture (Spondylolysis)
Location
Department of Orthopedics, Tokushima University, Tokushima, Japan 3-18-15 Kuramoto-cho, Tokushima-shi, Tokushima 770-8503, JAPAN
Access
Haneda airport to Tokushima airport (1 hour),
Tokushima airport to Tokushima Station (30 min, limousine bus),
Tokushima Station to Tokushima University Hospital (20 min, taxi)